Cocaine and related disorders

Definition
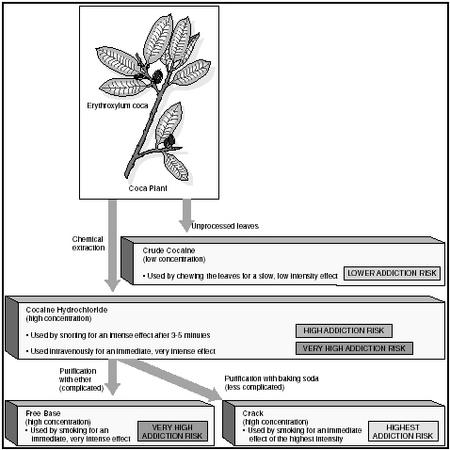
Cocaine is extracted from the coca plant, which grows in Central and South America. The substance is processed into many forms for use as an illegal drug of abuse. Cocaine is dangerously addictive, and users of the drug experience a "high"—a feeling of euphoria or intense happiness, along with hypervigilance, increased sensitivity, irritablity or anger, impaired judgment, and anxiety.
Forms of the drug
In its most common form, cocaine is a whitish crystalline powder that produces feelings of euphoria when ingested. In powder form, cocaine is known by such street names as "coke," "blow," "C," "flake," "snow" and "toot." It is most commonly inhaled or "snorted." It may also be dissolved in water and injected.
Crack is a form of cocaine that can be smoked and that produces an immediate, more intense, and more short-lived high. It comes in off-white chunks or chips called "rocks."
In addition to their stand-alone use, both cocaine and crack are often mixed with other substances. Cocaine may be mixed with methcathinone to create a "wildcat." Cigars may be hollowed out and filled with a mixture of crack and marijuana. Either cocaine or crack used in conjunction with heroin is called a "speedball." Cocaine used together with alcohol represents the most common fatal two-drug combination.
Description
Cocaine-related disorders is a very broad topic. According to the mental health clinician's handbook, Diagnostic and Statistical Manual of Mental Disorders , fourth edition, text revised (also known as the DSM-IV-TR ), the broad category of cocaine-related disorders can be subdivided into two categories: cocaine use disorders and cocaine-induced disorders. Cocaine use disorders include cocaine dependence and cocaine abuse. Cocaine-induced disorders include:
- cocaine intoxication
- cocaine withdrawal
- cocaine intoxication delirium
- cocaine-induced psychotic disorder, with delusions
- cocaine-induced psychotic disorder, with hallucinations
- cocaine-induced mood disorder
- cocaine-induced anxiety disorder
- cocaine-induced sexual dysfunction
- cocaine-induced sleep disorder
- cocaine-related disorder not otherwise specified
Cocaine use disorders
COCAINE ABUSE. For the cocaine abuser, the use of the substance leads to maladaptive behavior over a 12-month period. The person may fail to meet responsibilities at school, work, or home. The cocaine abuse impairs the affected person's judgment, and he or she puts him- or herself in physical danger to use the substance. For example, the individual may use cocaine in an unsafe environment. The person who abuses cocaine may be arrested or charged with possession of the substance, yet will continue to use cocaine despite all of the personal and legal problems that may result.
COCAINE DEPENDENCE. Cocaine dependence is even more serious than cocaine abuse. Dependence is a maladaptive behavior that, over a three-month period, has caused the affected individual to experience tolerance for and withdrawal symptoms from cocaine. Tolerance is the need to increase the amount of cocaine intake to achieve the same desired effect. In other words, someone who is dependent on cocaine needs more cocaine to produce the same "high" that a lesser amount produced in the past. The dependent person also experiences cocaine withdrawal. Withdrawal symptoms develop within hours or days after cocaine use that has been heavy and prolonged and then abruptly stopped. The symptoms include irritable mood and two or more of the following symptoms: fatigue , nightmares, difficulty sleeping or too much sleep, elevated appetite, agitation (restlessness), or slowed physical movements. The onset of withdrawal symptoms can cause a person to use more cocaine to avoid these painful and uncomfortable symptoms. The dependent person uses larger amounts of cocaine for longer periods of time than intended. He or she cannot cut back on the use of the substance, often has a difficult time resisting cocaine when it is available, and may abandon work or school to spend more time acquiring and planning to acquire more cocaine. The individual continues to use the cocaine despite the negative effects it has on family life, work, and school.
Cocaine-induced disorders
COCAINE INTOXICATION. Cocaine intoxication occurs after recent cocaine use. The person experiences a feeling of intense happiness, hypervigilance, increased sensitivity, irritability or anger, with impaired judgment, and anxiety. The intoxication impairs the person's ability to function at work, school, or in social situations. Two or more of the following symptoms are present immediately after the use of the cocaine:
- enlarged pupils
- elevated heart rate
- elevated or lowered blood pressure
- chills and increased sweating
- nausea or vomiting
- weight loss
- agitation or slowed movements
- weak muscles
- chest pain
- coma
- confusion
- irregular heartbeat
- depressed respiration
- seizures
- odd postures
- odd movements
COCAINE WITHDRAWAL. As mentioned, withdrawal symptoms develop within hours or days after cocaine use that has been heavy and prolonged and then abruptly stopped. The symptoms include irritable mood and two or more of the following symptoms: fatigue, nightmares, difficulty sleeping or too much sleep, elevated appetite, agitation (restlessness), or slowed physical movements.
COCAINE-INDUCED DELIRIUM. According to the DSM-IV-TR , several criteria must be met in order for a health care professional to establish the diagnosis of cocaine-induced delirium. Patients have a disturbance of their level of consciousness or awareness, evidenced by drowsiness or an inability to concentrate or pay attention. Patients also experience a change in their cognition (ability to think) evidenced by a deficit in their language or their memory. For example, these patients may forget where they have placed an item, or their speech is confusing. These symptoms have rapid onset within hours or days of using cocaine and the symptoms fluctuate throughout the course of the day. These findings cannot be explained by dementia (state of impaired thought processes and memory that can be caused by various diseases and conditions) and the doctor must not be able to recognize some other physical reason that can account for the symptoms other than cocaine intoxication.
COCAINE-INDUCED PSYCHOTIC DISORDER, WITH DELUSIONS. The person suffering from this disorder has experienced intoxication or withdrawal from cocaine within a month from the time he or she begins to experience delusions (beliefs that the person continues to maintain, despite evidence to the contrary). In order for this state to be considered cocaine-induced psychotic disorder, these symptoms cannot be due to another condition or substance.
COCAINE-INDUCED PSYCHOTIC DISORDER, WITH HALLUCINATIONS. This condition is the same as cocaine-induced psychotic disorder with delusions, except that this affected individual experiences hallucinations instead of delusions. Hallucinations can be described as hearing and seeing things that are not real.
COCAINE-INDUCED MOOD DISORDER. The person suffering from this disorder has experienced intoxication or withdrawal from cocaine within a month from the time
COCAINE-INDUCED ANXIETY DISORDER. The person suffering from this disorder has experienced intoxication or withdrawal from cocaine within a month from the time he or she begins to experience anxiety, panic attacks, obsessions, or compulsions. Panic attacks are discrete episodes of intense anxiety. Persons affected with panic attacks may experience accelerated heart rate, shaking or trembling, sweating, shortness of breath, or fear of going crazy or losing control, as well as other symptoms. An obsession is an unwelcome, uncontrollable, persistent idea, thought, image, or emotion that a person cannot help thinking even though it creates significant distress or anxiety. A compulsion is a repetitive, excessive, meaningless activity or mental exercise which a person performs in an attempt to avoid distress or worry.
COCAINE-INDUCED SEXUAL DYSFUNCTION. The person suffering from this disorder has experienced intoxication or withdrawal from cocaine within a month from the time he or she begins to experience sexual difficulties, and these difficulties are deemed by the clinician to be due directly to the cocaine use. Substance-induced sexual difficulties can range from impaired desire, impaired arousal, impaired orgasm, or sexual pain.
COCAINE-INDUCED SLEEP DISORDER. This disorder is characterized by difficulty sleeping ( insomnia ) during intoxication or increased sleep duration when patients are in withdrawal.
COCAINE-RELATED DISORDER NOT OTHERWISE SPECIFIED. This classification is reserved for clinicians to use when a cocaine disorder that the clinician sees does not fit into any of the above categories.
Causes and symptoms
Causes
BIOCHEMICAL/PHYSIOLOGICAL CAUSES. Twin studies have demonstrated that there is a higher rate of cocaine abuse in identical twins as compared to fraternal twins. This indicates that genetic factors contribute to the development of cocaine abuse. This finding also indicates, however, that unique environmental factors contribute to the development of cocaine abuse, as well. (If genes alone determined who would develop cocaine dependence, 100% of the identical twins with the predisposing genes would develop the disorder. However, because the results show only a relationship, or a correlation, between genetics and cocaine use among twins, these results indicate that other factors must be at work, as well.) Studies have also shown that disorders like attention-deficit/hyperactivity disorder (ADHD), conduct disorder , and anti-social personality disorder all have genetic components, and since patients who abuse cocaine have a high incidence of these diagnoses, they may also be genetically predisposed to abusing cocaine.
REINFORCEMENT. Learning and conditioning also play a unique role in the perpetuation of cocaine abuse. Each inhalation and injection of cocaine causes pleasurable feelings that reinforce the drug-taking procedure. In addition, the patient's environment also plays a role in cueing and reinforcing the experience in the patient's mind. The association between cocaine and environment is so strong that many people recovering from cocaine addiction report that being in an area where they used drugs brings back memories of the experience and makes them crave drugs. Specific areas of the brain are thought to be involved in cocaine craving, including the amygdala (a part of the brain that controls aggression and emotional reactivity), and the prefrontal cortex (a part of the brain that regulates anger, aggression, and the brain's assessment of fear, threats, and danger).
Symptoms
The following list is a summary of the acute (short-term) physical and psychological effects of cocaine on the body:
- blood vessels constrict
- elevated heart rate
- elevated blood pressure
- a feeling of intense happiness
- elevated energy level
- a state of increased alertness and sensory sensitivity
- elevated anxiety
- panic attacks
- elevated self-esteem
- diminished appetite
- spontaneous ejaculation and heightened sexual arousal
- psychosis (loss of contact with reality)
The following list is a summary of the chronic (long-term) physical and psychological effects of cocaine on the body:
- depressed mood
- irritability
- physical agitation
- decreased motivation
- difficulty sleeping
- hypervigilance
- elevated anxiety
- panic attacks
- hallucinations
- psychosis
Demographics
The patterns of cocaine abuse in the United States have changed much over the past thirty years. The patterns have also been changing in other parts of the world as well, including South America and Western Europe. In the United States, several studies have attempted to track drug abuse in many different populations. The studies include: the Monitoring the Future Study (MTF); the National Household Survey on Drug Abuse (NHSDA); the Drug Abuse Warning Network (DAWN), which gets reports from Emergency Rooms and medical examiners' offices on drug-related cases and deaths; and Arrestee Drug Abuse Monitoring (ADAM), which gets information on urine samples obtained from people who have been arrested.
In the annual MTF study, cocaine use among high school seniors had declined from 13.1% in 1985 to 3.1% in 1992—the lowest it had been since 1975 when the survey was first implemented. The rate of cocaine use began to rise again and peaked at 5.5% in 1997. The NHSDA found that the levels of cocaine use declined over the same time period. The decline in the rates has been thought to be due in part to education about the risks of cocaine abuse.
The incidence of new crack cocaine users has also decreased. There was a minimal decline in the numbers of excessive cocaine users between the years 1985 and 1997. The Epidemiologic Catchment Area (ECA) studies done in the early 1980s combined cocaine dependence with cocaine abuse and found that one-month to six-month prevalence rates for cocaine abuse and dependence were low or could not be measured. The lifetime rate of cocaine abuse was 0.2%.
A 1997 study from The National Institute on Drug Abuse indicates that among outpatients who abuse substances, 55% abuse cocaine.
Cocaine abuse affects both genders and many different populations across the United States. Males are one-and-a-half to two times more likely to abuse cocaine than females. Cocaine began as a drug of the upper classes in the 1970s; now the socioeconomic status of cocaine users has shifted. Cocaine is more likely to be abused by the economically disadvantaged because it is easy for them to get, and it is inexpensive ($10 for a small bag of crack cocaine). These factors have led to increased violence (because people who are cocaine dependent often will become involved in illegal activity, such as drug dealing, in order to acquire funds for their habit) and higher rates of acquired immune deficiency (AIDS) among disadvantaged populations.
Diagnosis
If a mental health clinician suspects cocaine use, he or she may ask the patient specifically about swallowing, injecting, or smoking the substance. Urine and blood testing will also be conducted to determine the presence of the substance. Doctors may also talk to friends or relatives concerning the patient's drug use, especially for cases in which the physician suspects that the patient is not being entirely honest about substance use. The clinician may also investigate a patient's legal history for drug arrests that may give clues to periods of substance abuse to which the patient will not admit.
Differential diagnosis
Differential diagnosis is the process of distinguishing one condition from other, similar conditions. The cocaine abuse disorder is easily confused with other substance abuse disorders and various forms of mental illness.
The symptoms of cocaine intoxication, such as increased talkativeness, poor sleep, and the intense feelings of happiness are similar to the symptoms for bipolar disorder , so the urine toxification screening test may play a key role in the diagnosis. Patients with cocaine intoxication with hallucinations and delusions can be mistaken for schizophrenic patients instead, further emphasizing the importance of the urine and blood screens. As part of establishing the diagnosis, the physician must also rule out PCP (phencyclidine) intoxication and Cushing's disease (an endocrine disorder of excessive cortisol production). Withdrawal symptoms are similar to those of the patient with major depression. For this reason, the clinician may ask the patient about his or her mood during times of abstinence from drug use to discern if any true mood disorders are present. If cocaine use is causing depression, the depression should resolve within a couple of weeks of stopping drug use.
Laboratory testing
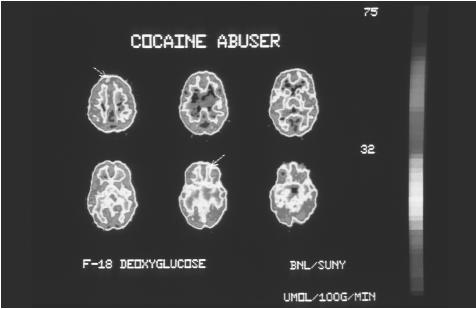
The breakdown products of cocaine remain in the urine. The length of time that they remain depends on the dose of cocaine, but most doses would not remain in the urine longer than a few days. Cocaine can also be found in other bodily fluids such as blood, saliva, sweat, and hair, and these provide better estimates as to recent cocaine use. The hair can hold evidence that a patient has been using drugs for weeks to months. Positron emission tomography (PET) and single-photon emission computed tomography (SPECT) are different kinds of imaging studies . Both kinds of scans look at the amount of blood that is flowing to the brain. When these images are taken of the brains of people who abuse cocaine, the resulting scans have revealed abnormalities in certain sections of the brain. The brains of people addicted to cocaine shrink, or atrophy.
Neuropsychological assessment
Neuropsychological testing is also an important tool for examining the effects of toxic substances on brain functioning. Some physicians may use neuropsychological assessments to reveal patients' cognitive and physical impairment after cocaine use. Neuropsychological testing assesses brain functioning through structured and systematic behavioral observation. Neuropsychological tests are designed to examine a variety of cognitive abilities, including speed of information processing, attention, memory, and language. An example of a task that a physician might ask the patient to complete as part of a neuropsychological examination is to name as many words beginning with a particular letter as the patient can in one minute. Patients who abuse cocaine often have difficulty completing tasks, such as the one described, that require concentration and memory.
Treatments
Psychological and social interventions
TREATMENT SETTINGS. Not all patients who abuse cocaine need to resort to long-term treatment. Treatment length varies with the degree that a person is dependent on the substance. If the patient has other psychiatric conditions such as major depression or schizophrenia or has significant medical complications of cocaine abuse, then he or she is more likely to require higher-intensity treatment. Residential programs/therapeutic communities may be helpful, particularly in more severe cases. Patients typically spend six to 12 months in such programs, which may also include vocational training and other features. The availability of such treatment, as well
PSYCHOTHERAPY. A wide range of behavioral interventions have been successfully used to treat cocaine addiction. The approach used must be tailored to the specific needs of each individual patient, however.
Contingency management rewards drug abstinence (confirmed by urine testing) with points or vouchers which patients can exchange for such things as an evening out or membership in a gym. Cognitive-behavioral therapy helps users learn to recognize and avoid situations most likely to lead to cocaine use and to develop healthier ways to cope with stressful situations.
Supportive therapy helps patients to modify their behavior by preventing relapse by taking actions such as staying away from drug-using friends and from neighborhoods or situations where cocaine is abundant.
Self-help groups like Narcotics Anonymous (NA) or Cocaine Anonymous (CA) are helpful for many recovering substance abusers. CA is a twelve-step program for cocaine abusers modeled after Alcoholics Anonymous (AA). Support groups and group therapy led by a therapist can be helpful because other addicts can share coping and relapse-prevention strategies. The group's support can help patients face devastating changes and life issues. Some experts recommend that patients be cocaine-free for at least two weeks before participating in a group, but other experts argue that a two-week waiting period is unnecessary and counterproductive. Group counseling sessions led by drug counselors who are in recovery themselves are also useful for some people overcoming their addictions. These group counseling sessions differ from group therapy in that the people in a counseling group are constantly changing.
The National Institute of Drug Abuse conducted a study comparing different forms of psychotherapy : patients who had both group drug counseling and individual drug counseling had improved outcomes. Patients who had cognitive-behavioral therapy stayed in treatment longer.
Medications
Many medications—greater than twenty—have been tested but none have been found to reduce the intensity of withdrawal. Dopamine agonists like amantadine and bromocriptine and tricyclic antidepressants such as desipramine have failed in studies to help treat symptoms of cocaine withdrawal or intoxication.
Alternative therapy
Alternative techniques, such as acupuncture , EEG biofeedback , and visualization, may be useful in treating addiction when combined with conventional treatment approaches.
Prognosis
Not all cocaine abusers become dependent on the drug. However, even someone who only uses occasionally can experience the harmful effects (interpersonal relationship conflicts, work or school difficulties, etc.) of using cocaine, and even occasional use is enough to addict. In the course of a person's battle with cocaine abuse, he or she may vary the forms of the drug that he or she uses. A person may use the inhaled form at one time and the injected form at another, for example.
Many studies of short-term outpatient treatment over a six-month to two-year period indicate that people addicted to cocaine have a better chance of recovering than people who are addicted to heroin. A study of veterans who participated in an inpatient or day hospital treatment program that lasted 28 days, revealed that about 60% of people who were abstinent at four months were able to maintain their abstinence at seven months.
Having a good social support network greatly improves the prognosis for recovery from cocaine abuse and dependence.
Prevention
Efforts to prevent cocaine abuse, as well as any substance abuse, begin with prevention programs that are based in schools, in the workplace, heath care clinics, criminal justice systems, and public housing. Programs such as Students Taught Awareness (STAR) are cost effective and have reduced the rates of substance abuse in the schools. These school-based programs also foster parental involvement and education about substance abuse issues. The juvenile justice system also implements drug prevention programs. Even many workplaces provide drug screening and treatment and counseling for those who test positive. Employers may also provide workshops on substance abuse prevention. The United States Department of Housing and Urban Development (HUD) also sponsors drug prevention programs.
Resources
BOOKS
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th edition, text revised. Washington, DC: American Psychiatric Association, 2000.
Jaffe, Jerome H., M.D. "Cocaine-Related Disorders." In Comprehensive Textbook of Psychiatry , edited by Benjamin J. Sadock, M.D. and Virginia A. Sadock, M.D. 7th edition. Philadelphia: Lippincott Williams and Wilkins, 2000.
Matthews, John. "Substance-Related Disorders: Cocaine and Narcotics." In Psychiatry Update and Board Preparation, edited by Thomas A. Stern, M.D. and John B. Herman, M.D. New York: McGraw Hill, 2000.
PERIODICALS
Adinoff, Byron, M.D. and others. "Limbic Response to Procaine in Cocaine Addicted Subjects." American Journal of Psychiatry March 2001: 390-398.
Held, Gale A., M.P.A. "Linkages Between Substance Abuse Prevention and Other Human Services Literature Review." National Institute on Drug Abuse (NIDA) June 1998.
Jacobsen, Leslie K., M.D. and others. "Quantitative Morphology of the Caudate and Putamen in Patients With Cocaine Dependence." American Journal of Psychiatry March 2000: 486-489.
Kampman, Kyle M., M.D. and others. "Amantadine in the Treatment of Cocaine-Dependent Patients With Severe Withdrawal Symptoms." American Journal of Psychiatry December 2000: 2052-2054.
ORGANIZATIONS
The American Academy of Addiction Psychiatry (AAAP). 7301 Mission Road, Suite 252, Prairie Village, KS, 66208. (913) 262-6161. <http://www.aaap.org > .
Cocaine Anonymous World Services (CAWS). 3740 Overland Ave. Ste. C, Los Angeles, CA, 90034. (310) 559-5833. <http://www.ca.org> .
National Institute on Drug Abuse (NIDA). 6001 Executive Boulevard, Room 5213, Bethesda, MD, 20892-9561.(301) 443-1124. <http://www.nida.nih.gov> .
OTHER
Leshner, Alan Ph.D. "Cocaine Abuse and Addiction." National Institute on Drug Abuse Research Report Series NIH Publication Number 99-4342, Washington, D.C. Supt.of doc. US. Govt. Print. Off., 1999.
Susan Hobbs, M.D.
Peter Gregutt
It is frightening to think that one can lose control of the ability to choose one's physical actions and behaviour and disregard it wit such lack of emotion.