Schizophrenia

Definition
Schizophrenia is the most chronic and disabling of the severe mental disorders, associated with abnormalities of brain structure and function, disorganized speech and behavior, delusions , and hallucinations . It is sometimes called a psychotic disorder or a psychosis .
Description
People diagnosed with schizophrenia do not always have the same set of symptoms; in addition, a given patient's symptoms may change over time. Since the nineteenth century, doctors have recognized different subtypes of the disorder, but no single classification system has gained universal acceptance. Some psychiatrists prefer to speak of schizophrenia as a group or family of disorders ("the schizophrenias") rather than as a single entity. A standard professional reference, The Diagnostic and Statistical Manual of Mental Disorders (also known as the DSM-IV-TR) acknowledges that its present classification of subtypes is not fully satisfactory for either clinical or research purposes, and states that "alternative subtyping schemes are being actively investigated."
The symptoms of schizophrenia can appear at any time after age six or seven, although onset during adolescence and early adult life is the most common pattern. There are a few case studies in the medical literature of schizophrenia in children younger than five, but they are extremely rare. Schizophrenia that appears after age 45 is considered late-onset schizophrenia. About 1%–2% of cases are diagnosed in patients over 80.
The onset of symptoms in schizophrenia may be either abrupt (sudden) or insidious (gradual). Often, however, it goes undetected for about two to three years after the onset of diagnosable symptoms, because the symptoms occur in the context of a previous history of cognitive and behavioral problems. The patient may have had panic attacks, social phobia , or substance abuse problems, any of which can complicate the process of diagnosis . In most cases, however, the patient's first psychotic episode is preceded by a prodromal (warning) phase, with a variety of behaviors that may include angry outbursts, withdrawal from social activities, loss of attention to personal hygiene and grooming, anhedonia (loss of one's capacity for enjoyment), and other unusual behaviors. The psychotic episode itself is typically characterized by delusions, which are false but strongly held beliefs that result from the patient's inability to separate real from unreal events; and hallucinations, which are disturbances of sense perception. Hallucinations can affect any of the senses, although the most common form of hallucination in schizophrenia is auditory ("hearing voices"). Autobiographical accounts by people who have recovered from schizophrenia indicate that these hallucinations are experienced as frightening and confusing. Patients often find it difficult to concentrate on work, studies, or formerly pleasurable activities because of the constant "static" or "buzz" of hallucinated voices.
There is no "typical" pattern or course of the disorder following the first acute episode. The patient may never have a second psychotic episode; others have occasional episodes over the course of their lives but can lead fairly normal lives otherwise. About 70% of patients diagnosed with schizophrenia have a second psychotic breakdown within five to seven years after the first one.
Some patients remain chronically ill; of these, some remain at a fairly stable level while others grow steadily worse and become severely disabled.
About 20% of patients with schizophrenia recover the full level of functioning that they had before the onset of the disorder, according to NIMH statistics; but the remaining 80% have problems reintegrating into mainstream society. These patients are often underachievers in school and in the workplace, and they usually have difficulty forming healthy relationships with others. The majority (60%–70%) of patients with schizophrenia do not marry or have children, and most have very few friends or social contacts. The impact of these social difficulties as well as the stress caused by the symptoms themselves is reflected in the high suicide rate among patients with schizophrenia. About 10% commit suicide within the first 10 years after their diagnosis— a rate 20 times higher than that of the general population.
Subtypes of schizophrenia
DSM-IV-TR specifies five subtypes of schizophrenia:
- Paranoid type. The central feature of this subtype is the presence of auditory hallucinations or delusions alongside relatively unaffected mood and cognitive functions. The patient's delusions usually involve persecution, grandiosity, or both. About a third of patients diagnosed with schizophrenia in the United States belong to this subtype.
- Disorganized type. The core features of this subtype include disorganized speech, disorganized behavior, and flat or inappropriate affect. The person may lose the ability to perform most activities of daily living, and may also make faces or display other oddities of behavior. This type of schizophrenia was formerly called hebephrenic (derived from the Greek word for puberty), because some of the patients' behaviors resemble adolescent silliness.
- Catatonic type. Catatonia refers to disturbances of movement, whether remaining motionless for long periods of time or excessive and purposeless movement. The absence of movement may take the form of catalepsy, which is a condition in which the patient's body has a kind of waxy flexibility and can be repositioned by others; or negativism, a form of postural rigidity in which the patient resists being moved by others. A catatonic patient may assume bizarre postures or imitate the movements of other people.
- Undifferentiated type. Patients in this subtype have some of the characteristic symptoms of schizophrenia but do not meet the full criteria for the paranoid, disorganized, or catatonic subtypes.
- Residual type. Patients in this category have had at least one psychotic episode, continue to have some negative symptoms of schizophrenia, but do not have current psychotic symptoms.
Cultural variables
There appear to be some differences across cultures in the symptoms associated with schizophrenia. The catatonic subtype appears to be more common in non-Western countries than in Europe or North America. Other studies indicate that persons diagnosed with schizophrenia in developing countries have a more acute onset of the disorder but better outcomes than patients in the developed countries.
Causes and symptoms
Causes
As of 2002, schizophrenia is considered the end result of a combination of genetic, biochemical, developmental, and environmental factors, some of which are still not completely understood. There is no known single cause of the disorder.
GENETIC. Researchers have known for many years that first-degree biological relatives of patients with schizophrenia have a 10% risk of developing the disorder, as compared with 1% in the general population. The monozygotic (identical) twin of a person with schizophrenia has a 40%–50% risk. The fact that this risk is not higher, however, indicates that environmental as well as genetic factors are implicated in the development of schizophrenia.
Some specific regions on certain human chromosomes have been linked to schizophrenia. In late 2001, a multidisciplinary team of researchers reported positive associations for schizophrenia on chromosomes 15 and 13. Chromosome 15 is linked to schizophrenia in European-American families as well as some Taiwanese and Portuguese families. A recent study of the biological pedigrees found among the inhabitants of Palau (an isolated territory in Micronesia) points to chromosomes 2 and 13. Still another team of researchers has suggested that a disorder known as 22q deletion syndrome may actually represent a subtype of schizophrenia, insofar as people with this syndrome have a 25% risk of developing schizophrenia. At present scientists are inclined to think that the genetic factors underlying schizophrenia vary across different ethnic groups, so that it is highly unlikely that susceptibility to the disorder is determined by only one gene. As of 2002, schizophrenia is considered a polygenic disorder.
There appears to be a connection between aging and genetic mutations that increases susceptibility to schizophrenia. A recent Israeli study found that the age of a person's father is a risk factor for schizophrenia; the older the father, the higher the rate of mutations in sperm cells. The child of a father older than 50 is three times more likely to develop schizophrenia than children born to younger men. The researchers suggest that mutations in the sperm cells of older men help to explain why schizophrenia has persisted in the human population even though few schizophrenics marry and have children.
DEVELOPMENTAL. As of 2002, there is some evidence that schizophrenia may be a type of developmental disorder related to the formation of faulty connections between nerve cells during fetal development. The changes in the brain that normally occur during puberty then interact with these connections to trigger the symptoms of the disorder. Other researchers have suggested that a difficult childbirth may result in developmental vulnerabilities that eventually lead to schizophrenia.
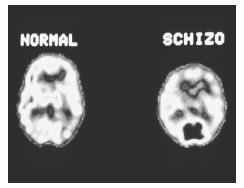
NEUROBIOLOGICAL. In early 2002, researchers at the NIMH demonstrated the existence of a connection between two abnormalities of brain functioning in patients with schizophrenia. The researchers used radioactive tracers and positron emission tomography (PET) to show that reduced activity in a part of the brain called the prefrontal cortex was associated in the patients, but not in the control subjects, with abnormally elevated levels of dopamine in the striatum. High levels of dopamine are related to the delusions and hallucinations of psychotic episodes in schizophrenia. The findings suggest that treatment directed at the prefrontal cortex might be more effective than present antipsychotic medications, which essentially target dopamine levels without regard to specific areas of the brain.
Another area of investigation concerns abnormalities in brain structure that are found in some patients with schizophrenia. One of these abnormalities is the increased size of the ventricles, which are cavities in the interior of the brain filled with cerebrospinal fluid. Another is a decrease in size of some areas of the brain. A California study of MRI scans of teenagers with early-onset schizophrenia found that they lost over 10% of the gray matter of the brain over the course of five years. The frontal eye fields showed the most rapid rate of tissue loss—about 5% per year. A major difficulty in interpreting these findings is that these abnormalities are not found in the brains of all patients with schizophrenia. In addition, they sometimes occur in the brains of people who do not have the disorder.
ENVIRONMENTAL. Certain environmental factors during pregnancy are associated with an increased risk of schizophrenia in the offspring. These include the mother's exposure to starvation or famine; influenza during the second trimester of pregnancy; and Rh incompatibility in a second or third pregnancy.
Some researchers are investigating a possible connection between schizophrenia and viral infections of the hippocampus, a structure in the brain that is associated with memory formation and the human stress response. It is thought that damage to the hippocampus might account for the sensory disturbances found in schizophrenia. Another line of research related to viral causes of schizophrenia concerns a protein deficiency in the brain. Researchers at the University of Kiel in Germany think that the deficiency is the result of viral infections.
Environmental stressors related to home and family life (parental death or divorce, family dysfunction) or to separation from the family of origin in late adolescence (going away to college or military training; marriage) may trigger the onset of schizophrenia in individuals with genetic or psychological vulnerabilities.
Symptoms
The symptoms of schizophrenia are divided into two major categories: positive symptoms , which are defined by DSM-IV-TR as excesses or distortions of normal mental functions; and negative symptoms , which represent a loss or reduction of normal functioning. Of the two types, the negative symptoms are more difficult to evaluate because they may be influenced by a concurrent depression or a dull and unstimulating environment, but they account for much of the morbidity (unhealthiness) associated with schizophrenia.
POSITIVE SYMPTOMS. The positive symptoms of schizophrenia include four so-called "first-rank" or Schneiderian symptoms, named for a German psychiatrist who identified them in 1959:
- Delusions. A delusion is a false belief that is resistant to reason or to confrontation with actual facts. The most common form of delusion in patients with schizophrenia is persecutory; the person believes that others— family members, clinical staff, terrorists, etc.—are "out to get" them. Another common delusion is referential, which means that the person interprets objects or occurrences in the environment (a picture on the wall, a song played on the radio, laughter in the corridor, etc.) as being directed at or referring to them.
- Somatic hallucinations. Somatic hallucinations refer to sensations or perceptions about one's body organs that have no known medical cause, such as feeling that snakes are crawling around in one's intestines or that one's eyes are emitting radioactive rays.
- Hearing voices commenting on one's behavior or talking to each other. Auditory hallucinations are the most common form of hallucination in schizophrenia, although visual, tactile, olfactory, and gustatory hallucinations may also occur. Personal accounts of recovery from schizophrenia often mention "the voices" as one of the most frightening aspects of the disorder.
- Thought insertion or withdrawal. These terms refer to the notion that other beings or forces (God, aliens from outer space, the CIA, etc.) can put thoughts or ideas into one's mind or remove them.
Other positive symptoms of schizophrenia include:
- Disorganized speech and thinking. A person with schizophrenia may ramble from one topic to another (derailment or loose associations); may give unrelated answers to questions (tangentiality); or may say things that cannot be understood because there is no grammatical structure to the language ("word salad" or incoherence).
- Disorganized behavior. This symptom includes such behaviors as agitation; age-inappropriate silliness; inability to maintain personal hygiene; dressing inappropriately for the weather; sexual self-stimulation in public; shouting at people, etc. In one case study, the patient played his flute for hours on end while standing on top of the family car.
- Catatonic behavior. Catatonic behaviors have been described with regard to the catatonic subtype of schizophrenia. This particular symptom is sometimes found in other mental disorders.
NEGATIVE SYMPTOMS. The negative symptoms of schizophrenia include:
- Blunted or flattened affect. This term refers to loss of emotional expressiveness. The person's face may be unresponsive or expressionless, and speech may lack vitality or warmth.
- Alogia. Alogia is sometimes called poverty of speech. The person has little to say and is not able to expand on their statements. A doctor examining the patient must be able to distinguish between alogia and unwillingness to speak.
- Avolition. The person is unable to begin or stay with goal-directed activities. They may sit in one location for long periods of time or show little interest in joining group activities.
- Anhedonia. Anhedonia refers to the loss of one's capacity for enjoyment or pleasure.
OTHER SYMPTOMS AND CHARACTERISTICS. Although the following symptoms and features are not diagnostic criteria of schizophrenia, most patients with the disorder have one or more:
- Dissociative symptoms, particularly depersonalization and derealization.
- Anosognosia. This term originally referred to the inability of stroke patients to recognize their physical disabilities, but is sometimes used to refer to lack of insight in patients with schizophrenia. Anosognosia is associated with higher rates of noncompliance with treatment, a higher risk of repeated psychotic episodes, and a poorer prognosis for recovery.
- High rates of substance abuse disorders. About 50% of patients diagnosed with schizophrenia meet criteria for substance abuse or dependence. While substance abuse does not cause schizophrenia, it can worsen the symptoms of the disorder. Patients may have particularly bad reactions to amphetamines , cocaine, PCP ("angel dust") or marijuana. It is thought that patients with schizophrenia are attracted to drugs of abuse as self-medication for some of their symptoms. The most common substance abused by patients with schizophrenia is tobacco; 90% of patients are heavy cigarette smokers, compared to 25%–30% in the general adult population. Smoking is a serious problem for people with schizophrenia because it interferes with the effectiveness of their antipsychotic medications as well as increasing their risk of lung cancer and other respiratory diseases.
- High risk of suicide . About 40% of patients with schizophrenia attempt suicide at least once, and 10% eventually complete the act.
- High rates of obsessive-compulsive disorder and panic disorder.
- Downward drift. Downward drift is a sociological term that refers to having lower levels of educational achievement and/or employment than one's parents.
VIOLENT BEHAVIOR. The connection between schizophrenia and personal assault or violence deserves mention because it is a major factor in the reactions of family members and the general public to the diagnosis. Researchers in both the United Kingdom and the United States have found that schizophrenia carries a heavier stigma than most other mental disorders, largely because of the mass media's fascination with bizarre murders, dismemberment of animals, or other gruesome acts committed by people with schizophrenia. Many patients report that the popular image of a schizophrenic as "a time bomb waiting to explode" is a source of considerable emotional stress.
Risk factors for violence in a patient diagnosed with schizophrenia include male sex, age below 30, prediagnosis history of violence, paranoid subtype, nonadherence to medication regimen, and heavy substance abuse. On the other hand, it should be noted that most crimes of violence are committed by people without a diagnosis of schizophrenia. In addition, a study of patients with schizophrenia living in the community found that "... individuals in this sample were at least 14 times more likely to be victims of a violent crime than to be arrested for one."
Demographics
In the United States, Canada, and Western Europe, the sex ratio in schizophrenia is 1.2:1, with males being affected slightly more often than females. There is a significant gender difference in average age at onset, however; the average for males is between ages 18 and 25, whereas for women there are two peaks, one between ages 25 and 35, and a second rise in incidence after age 45. About 15% of all women who develop schizophrenia are diagnosed after age 35. In some women, the first symptoms of the disorder appear postpartum (after giving birth). Many women with schizophrenia are initially misdiagnosed as having depression or bipolar disorder , because women with schizophrenia are likely to have more difficulties with emotional regulation than men with the disorder. In general, however, females have higher levels of functioning prior to symptom onset than males.
The incidence of schizophrenia in the United States appears to be uniform across racial and ethnic groups, with the exception of minority groups in urban neighborhoods in which they are a small proportion of the total population. A recent study done in the United Kingdom replicated American findings: there are significantly higher rates of schizophrenia among racial minorities living in large cities. The rates of schizophrenia are highest in areas in which these minority groups form the smallest proportion of the local population. The British study included Africans, Caribbeans of African descent, and Asians.
The incidence of schizophrenia in most developed countries appears to be higher among people born in cities than among those born in rural areas. In addition, there appears to be a small historical/generational factor, with the incidence of schizophrenia gradually declining in later-born groups.
Schizophrenia is a leading cause of disability, not only in the United States, but in other developed countries around the world. In 1997, the World Health Organization (WHO) listed schizophrenia as the world's ninth leading cause of disability. According to the National Institute of Mental Health (NIMH), 2.2 million American adults, or 1.1% of the population over age 18, suffer from schizophrenia. Other estimates run as high as 1.5% of the population.
Schizophrenia is disproportionately costly to society for reasons that go beyond the sheer number of people affected by the disorder. Although patients with schizophrenia are little more than 1% of the population, they account for 2.5% of all health care costs—$40 billion per year in the United States, $2.35 billion in Canada (in Canadian dollars), and 2.6 billion pounds sterling (about $7.28 billion in US dollars) in Great Britain. In the United States, patients with schizophrenia fill 25% of all hospital beds and account for about 20% of all Social Security disability days.
In addition, the onset of the disorder typically occurs during a young person's last years of high school or their first years in college or the workforce; thus it often destroys their long-term plans for their future. According to the federal Agency for Healthcare Research and Quality, 70%–80% of people diagnosed with schizophrenia are either unemployed or underemployed (working in jobs well below their actual capabilities). Ten percent of Americans with permanent disabilities have schizophrenia, as well as 20%–30% of the homeless population.
Diagnosis
There are no symptoms that are unique to schizophrenia and no single symptom that is a diagnostic hallmark of the disorder. In addition, as of 2002 there are no laboratory tests or imaging studies that can establish or confirm a diagnosis of schizophrenia. The diagnosis is based on a constellation or group of related symptoms that are, according to DSM-IV-TR, "associated with impaired occupational or social functioning."
As part of the process of diagnosis, the doctor will take a careful medical history and order laboratory tests of the patient's blood or urine in order to rule out general
The doctor must then rule out other mental disorders that may be accompanied by psychotic symptoms, such as mood disorders; brief psychotic disorders; dissociative disorder not otherwise specified or dissociative identity disorder ; delusional disorder ; schizotypal, schizoid, or paranoid personality disorders ; and pervasive developmental disorders . In children, childhood-onset schizophrenia must be distinguished from communication disorders with disorganized speech and from attention-deficit/hyperactivity disorder .
After the doctor has ruled out other organic and mental disorders, he or she must then determine whether the patient meets the following criteria, as specified by DSM-IV-TR :
- Presence of positive and negative symptoms. The patient must have two (or more) of the following symptoms during a one-month period: delusions; hallucinations; disorganized speech; disorganized or catatonic behavior; negative symptoms.
- Decline in social, interpersonal, or occupational functioning, including personal hygiene or self-care.
- Duration. The symptomatic behavior must last for at least six months.
Treatments
Current treatment of schizophrenia focuses on symptom reduction and relapse prevention, since the causes of the disorder have not yet been clearly identified. Unfortunately, not all patients with schizophrenia receive adequate treatment. In 2000, the NIMH released the results of a large-scale community study, which indicated that fewer than half of patients with schizophrenia receive correct dosages of their medications or adequate psychosocial treatment.
Medications
Medications are the mainstay of treatment for schizophrenia. Drug therapy for the disorder, however, is complicated by several factors: the unpredictability of a given patient's response to specific medications, the number of potentially troublesome side effects, the high rate of substance abuse among patients with schizophrenia, and the possibility of drug interactions between antipsychotic medications and antidepressants or other medications that may be prescribed for the patient.
NEUROLEPTICS. The first antipsychotic medications for schizophrenia were introduced in the 1950s, and known as dopamine antagonists, or DAs. They are sometimes called neuroleptics, and include haloperidol (Haldol), chlorpromazine (Thorazine), perphenazine (Trilafon), and fluphenazine (Prolixin). About 40% of patients, however, fail to respond to treatment with these medications. Neuroleptics can control most of the positive symptoms of schizophrenia as well as reduce the frequency and severity of relapses but they have little effect on negative symptoms. In addition, these medications have problematic side effects, ranging from dry mouth, blurry vision, and restlessness (akathisia) to such long-term side effects as tardive dyskinesia (TD). TD is a disorder characterized by involuntary movements of the mouth, lips, arms, or legs; it affects about 15%–20% of patients who have been receiving neuroleptic medications over a period of years. Discomfort related to these side effects is one reason why 40% of patients treated with the older antipsychotics do not adhere to their medication regimens.
ATYPICAL ANTIPSYCHOTICS. The atypical antipsychotics are newer medications introduced in the 1990s. They are sometimes called serotonin dopamine antagonists, or SDAs. These medications include clozapine (Clozaril), risperidone (Risperdal), quetiapine (Seroquel), ziprasidone (Geodon), and olanzapine (Zyprexa). These newer drugs are more effective in treating the negative symptoms of schizophrenia and have fewer side effects than the older antipsychotics. Clozapine has been reported to be effective in patients who do not respond to neuroleptics, and to reduce the risk of suicide attempts. The atypical antipsychotics, however, do have weight gain as a side effect; and patients taking clozapine must have their blood monitored periodically for signs of agranulocytosis, or a drop in the number of white blood cells. These drugs are now considered first-line treatments for patients having their first psychotic episode.
OTHER PRESCRIPTION MEDICATIONS. Patients with schizophrenia have a lifetime prevalence of 80% for major depression; others suffer from phobias or other anxiety disorders. The doctor may prescribe antidepressants or a short course of benzodiazepines along with antipsychotic medications.
Inpatient treatment
Patients with schizophrenia are usually hospitalized during acute psychotic episodes, to prevent harm to themselves or to others, and to begin treatment with antipsychotic medications. A patient having a first psychotic episode is usually given a computed tomography (CT) or magnetic resonance imaging (MRI) scan to rule out structural brain disease.
Outpatient treatment
In recent years, patients with schizophrenia who have been stabilized on antipsychotic medications have been given psychosocial therapies of various types to assist them with motivation, self-care, and forming relationships with others. In addition, because many patients have had their education or vocational training interrupted by the onset of the disorder, they may be helped by therapies directed toward improving their social functioning and work skills.
Specific outpatient treatments that have been used with patients with schizophrenia include:
- Rehabilitation programs. These programs may offer vocational counseling, job training, problem-solving and money management skills, use of public transportation, and social skills training .
- Cognitive-behavioral therapy and supportive psychotherapy .
- Family psychoeducation . This approach is intended to help family members understand the patient's illness, cope with the problems it creates for other family members, and minimize stresses that may increase the patient's risk of relapse.
- Self-help groups . These groups provide mutual support for family members as well as patients. They can also serve as advocacy groups for better research and treatment, and to protest social stigma and employment discrimination.
Alternative and complementary therapies
Alternative and complementary therapies that are being investigated for the treatment of schizophrenia include gingko biloba , an Asian shrub, and vitamin therapy. One Chinese study reported that a group of patients who had not responded to conventional antipsychotic medications benefited from a thirteen-week trial of gingko extract, with significantly fewer side effects. Vitamin therapy is recommended by naturopathic practitioners on the grounds that many hospitalized patients with schizophrenia suffer from nutritional deficiencies. The supplements recommended include folic acid, niacin, vitamin B 6 , and vitamin C.
Prognosis
The prognosis for patients diagnosed with schizophrenia varies. About 20% recover their previous level of functioning, while another 10% achieve significant and lasting improvement. About 30%–35% show some improvement with intermittent relapses and some disabilities, while the remainder are severely and permanently incapacitated. Factors associated with a good prognosis include relatively good functioning prior to the first psychotic episode; a late or sudden onset of illness; female sex; treatment with antipsychotic medications shortly after onset; good compliance with treatment; a family history of mood disorders rather than schizophrenia; minimal cognitive impairment; and a diagnosis of paranoid or nondeficit subtype. Factors associated with a poor prognosis include early age of onset; a low level of prior functioning; delayed treatment; heavy substance abuse; noncompliance with treatment; a family history of schizophrenia; and a diagnosis of disorganized or deficit subtype with many negative symptoms.
Prevention
The multifactorial and polygenic etiology (origins or causes) of schizophrenia complicates the search for preventive measures against the disorder. It is possible that the complete mapping of the human genome will identify a finite number of genes that contribute to susceptibility to schizophrenia. The NIMH has presently compiled the world's largest registry of families affected by schizophrenia in order to pinpoint specific genes for further study. The NIMH also sponsors a Prevention Research Initiative to identify points in the development of schizophrenia at which patients could benefit from the application of preventive efforts.
Resources
BOOKS
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th edition, text revised. Washington, DC: American Psychiatric Association,2000.
Friedrich, Otto. Going Crazy: An Inquiry Into Madness in Our Time. New York: Avon Books, 1977.
Martin, John H., PhD. Neuroanatomy: Text and Atlas. Second edition. Norwalk, CT: Appleton and Lange, 1996.
North, Carol S., MD. Welcome Silence: My Triumph Over Schizophrenia. New York: Simon and Schuster, Inc.,1989.
Pelletier, Kenneth R., MD. "CAM Therapies for Specific Conditions: Schizophrenia." In The Best Alternative Medicine , Part II. New York: Simon and Schuster, 2002.
"Schizophrenia and Related Disorders." Section 15, Chapter 193 in The Merck Manual of Diagnosis and Therapy, edited by Mark H. Beers, MD, and Robert Berkow, MD. Whitehouse Station, NJ: Merck Research Laboratories, 2001.
Wahl, Otto F. Telling Is Risky Business: Mental Health Consumers Confront Stigma. New Brunswick, NJ: Rutgers University Press, 1999.
PERIODICALS
AACAP Council. "Practice Parameter for the Assessment and Treatment of Children and Adolescents with Schizophrenia." Journal of the American Academy of Child and Adolescent Psychiatry 40 (July 2001 Supplement): 4S–23S.
Barrowclough, Christine, Gillian Haddock, Nicholas Tarrier, and others. "Randomized Controlled Trial of Motivational Interviewing, Cognitive Behavior Therapy, and Family Intervention for Patients with Comorbid Schizophrenia and Substance Use Disorders." American Journal of Psychiatry 158 (October 2001): 1706–1713.
Bassett, A. S., S. O'Neill, J. Murphy, and others. "Expression of Schizophrenic Symptoms in 22q Deletion Syndrome." American Journal of Human Genetics 69 (October2001): 287.
Bower, Bruce. "Back from the Brink (Therapies for Schizophrenia)." Science News 159 (April 28, 2001): 268.
Boydell, J., J. van Os, K. McKenzie, and others. "Incidence of Schizophrenia in Ethnic Minorities in London: Ecological Study Into Interactions With the Environment." British Medical Journal 323 (December 8, 2001): 1336–1338.
Brekke, John S. "Risks for Individuals with Schizophrenia Who Are Living in the Community." Journal of the American Medical Association 286 (December 19, 2001): 2922.
Camp, Nicola J., Susan L. Neuhausen, Josepha Tiobech, and others. "Genomewide Multipoint Linkage Analysis of Seven Extended Palauan Pedigrees with Schizophrenia, by a Markov-Chain Monte Carlo Method." American Journal of Human Genetics 69 (December 2001): 1278–1289.
"Consider Clozapine for Reducing Suicide Risk in Schizophrenia." Clinical Psychiatry News 29 (November2001): 22.
Cormac, I., C. Jones, C. Campbell. "Cognitive Behaviour Therapy for Schizophrenia (Cochrane Review)." Cochrane Database Systems Review (2002): CD000524.
Fisher, Daniel B. "Recovering from Schizophrenia." (Guest Editorial). Clinical Psychiatry News 29 (November 2001): 30.
Frangou, Sophia. "How to Manage the First Episode of Schizophrenia: Early Diagnosis and Treatment May Prevent Social Disability Later." British Medical Journal 321 (September 2, 2000): 522.
Jancin, Bruce. "Women Often Defy Schizophrenia's Classic Course." Clinical Psychiatry News 29 (October 2001): 30.
Lehman, A. F., R. Goldberg, L. B. Dixon, and others. "Improving Employment Outcomes for Persons with Severe Mental Illness." Archives of General Psychiatry 59 (February 2002): 165–172.
McGrath, John. "Treatment of Schizophrenia." British Medical Journal 319 (October 16, 1999): 1045–1083.
"MRI Reveals Brain Changes Associated with Schizophrenia." Mental Health Weekly 11 (October 1,2001): 8.
Myin-Germeys I., L. Krabbendam, J. Jolles, and others. "Are Cognitive Impairments Associated with Sensitivity to Stress in Schizophrenia? An Experience Sampling Study." American Journal of Psychiatry 159 (March 2002): 443–449.
Nakaya, M., K. Kusumoto, K. Ohmori. "Subjective Experiences of Japanese Inpatients with Chronic Schizophrenia." Journal of Nervous and Mental Disorders 190 (February 2002): 80–85.
"Old Fathers and Schizophrenia." Harvard Mental Health Letter 18 (October 2001).
Ross, Brendan. "Novel Antipsychotic Drugs in the Management of Schizophrenia." Drug Topics (May 7,2001): 72–84.
"Schizophrenia May Be Linked to Brain Protein Deficiency." Mental Health Weekly 11 (November 19, 2001): 7.
Swofford, Cheryl D. "Double Jeopardy: Schizophrenia and Substance Abuse." American Journal of Drug and Alcohol Abuse 26 (August 2000): 343.
Weiser, Mark, Avraham Reichenberg, Jonathan Rabinowitz, and others. "Association Between Nonpsychotic Psychiatric Diagnoses in Adolescent Males and Subsequent Onset of Schizophrenia." Archives of General Psychiatry 58 (October 2001): 959–964.
Werbach, Melvyn R. "Vitamins for Treating Schizophrenia." Townsend Letter for Doctors and Patients (April 2001): 55–60.
ORGANIZATIONS
American Academy of Child and Adolescent Psychiatry. 3615 Wisconsin Avenue, NW, Washington, DC 20016-3007.(202) 966-7300. Fax: (202) 966-2891. <www.aacap.org> .
The National Alliance for the Mentally Ill (NAMI). 200 North Glebe Road, Suite 1015, Arlington, VA 22203-3754.(800) 950-NAMI or (703) 524-7600. <www.nami.org> .
National Alliance for Research on Schizophrenia and Depression (NARSAD). 60 Cutter Mill Road, Suite 404, Great Neck, NY 11021. (516) 829-0091. <www.mhsource.com> .
National Institute of Mental Health. 6001 Executive Boulevard, Room 8184, MSC 9663, Bethesda, MD 20892-9663. (301) 443-4513. <www.nimh.nih.gov> .
National Mental Health Association (NMHA). 1021 Prince Street, Alexandria, VA 22314-2971. (800) 969-6942 or(703) 684-7722. <www.nmha.org> .
OTHER
National Institute of Mental Health (NIMH). The Numbers Count. NIH Publication No. 01-4584 (2000). <www.nimh.nih.gov/publicat/numbers.cfm> .
National Institutes of Health (NIH). News Release, January 28, 2002. "Scans Link 2 Key Pieces of Schizophrenia Puzzle." <www.nih.gov/news/pr/jan2002/nimh-28.htm> .
Rebecca J. Frey, Ph.D.
Comment about this article, ask questions, or add new information about this topic: