Trichotillomania
Definition
Individuals with trichotillomania repetitively pull out their own hair. Trichotillomania as an impulse-control disorder. Some researchers view it as a type of affective or obsessive-compulsive disorder . Nail-biting, skin-picking, and thumb-sucking are considered to be related conditions.
Description
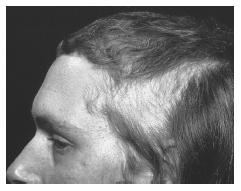
Trichotillomania involves hair-pulling episodes that result in noticeable hair loss. Although any area of the body can be a target, the most common areas are the scalp, followed by the eyelashes, eyebrows, and pubic region. Hair-pulling can occur without the individual's awareness, but is frequently preceded by a sense of increasing tension and followed by a sense of relief or gratification. The resulting hair loss can be a source of embarrassment or shame. Because of a tendency to hide symptoms, and because professionals are relatively unfamiliar with the disorder, individuals either may not seek, or are offered treatment. Untreated trichotillomania can result in impaired social functioning and medical complications.
Causes and symptoms
Causes
Scientific research regarding trichotillomania has been conducted primarily in the past 10 years and causes are only theoretical. Psychoanalytic theories suggest that the behavior is a way of dealing with unconscious conflicts or childhood trauma (such as sexual abuse ). Biological theories look for a genetic basis. For instance, people with trichotillomania often have a first-degree relative with an obsessive-compulsive spectrum disorder. Researchers are also evaluating similarities between trichotillomania and Tourette's disorder. Behavioral theories assume that symptoms are learned, that a child may imitate a parent who engages in hair-pulling. The behavior may also be learned independently if it serves a purpose. For example, hair-pulling may begin as a response to stress and then develop into a habit.
Symptoms
According to the Diagnostic and Statistical Manual of Mental Disorders , ( DSM-IV-TR ), produced by the American Psychiatric Association and used by most mental health professionals in North America and Europe to diagnose mental disorders, the following conditions must be present for a diagnosis of trichotillomania:
- noticeable hair loss (alopecia) due to recurrent hair-pulling
- tension immediately before hair-pulling, or when attempting to resist hair-pulling
- reduction of tension, or a feeling of pleasure or gratification, immediately following hair-pulling
- significant distress or impairment in social, occupational, or other important areas of functioning
In addition, the DSM-IV-TR requires that hair-pulling not be due to another medical or mental disorder. The tension-release requirement is controversial because 17% of people who otherwise qualify for this diagnosis do not experience this.
Symptoms usually emerge in early adolescence. Episodes may last a few minutes or a few hours during periods of stress or relaxation. Hairs with unique textures or qualities may be preferred. The pulling may include rituals, such as twirling hair off or examining the root. Half of those individuals with trichotillomania engage in oral behaviors—running hair across the lips or through the teeth, biting off the root (trichophagy), or eating hair (trichophagia). The usually try to control their behavior in the presence of others and may hide the affected areas. Symptoms may come and go for weeks, months, or years at a time.
Demographics
Once regarded as rare, trichotillomania is now considered more common, affecting 1–4% of people in the general population. When the tension-release requirement is excluded, trichotillomania occurs in adult females (3.4%) more often than adult males (1.5%). Among children, both genders are affected equally.
Diagnosis
Other possible causes of symptoms must first be ruled out. Hair loss may have a medical cause, such as a dermatological condition. Hair-pulling may have another
Severity of symptoms is also important. Twisting or playing with hair when nervous does not qualify as trichotillomania. If symptoms are minor or undetectable, a diagnosis should be given only if the individual expresses significant distress. Children should be given the diagnosis only if symptoms persist because hair-pulling may be a temporary phase, much like thumb-sucking.
If individuals deny symptoms, hair-pulling behavior can be assessed by objective measures such as the presence of short, broken hairs or damaged follicles. Some psychological assessment instruments are also available.
Treatments
Treatment usually starts by determining the current frequency and severity of symptoms. This information, which serves as a measure of progress, is gathered by (a) self-report; (b) reports from significant others; (c) objective measures, such as saving pulled hairs, videotapes, or measuring areas of hair loss; or (d) a combination of these methods.
Primarily, three categories of therapy have been used in the treatment of trichotillomania:
- Psychoanalysis focuses on childhood experiences and unresolved conflicts during early development.
- Medications. Those typically used are antidepressants with serotonergic properties (also used with obsessive-compulsive disorders). Clomipramine (Anafranil) has proven most effective. The selective serotonin reuptake inhibitors (SSRIs) have had mixed results. Some researchers recommend low doses of antipsychotic drugs (neuroleptics) in conjunction with SSRIs. Medications are usually combined with behavior therapy.
- Behavior therapy. This includes a number of different approaches: Punishment procedures such as electric shock, topical cream to enhance pain, or mittens placed on the person's hands, are effective but controversial. They are intrusive and are often used with individuals who may be unable to consent, such as children or people with developmental disabilities. Habit-reversal training is the most accepted approach. It teaches individuals to monitor their hair-pulling and substitute it for more healthy behaviors. Alternative forms of behavior therapy include biofeedback and hypnosis.
Prognosis
The effects of trichotillomania can be very serious: Associated feelings of shame may result in avoidance of social situations; chewing hair can result in dental erosion; eating hair may result in hairballs (trichobezoars) becoming lodged in the stomach or large intestine, which can lead to anemia, abdominal pain, nausea and vomiting, hematemesis (vomiting blood), or bowel obstruction or perforation.
Studies show low success rates with medications and traditional psychoanalysis. Behavioral therapy has reported long-term success rates of 90% or better. Follow-up sessions are encouraged to prevent relapse. A major issue in prognosis is whether an individual receives treatment. Professionals may not recognize or know how to treat trichotillomania effectively. Conversely, individuals with the disorder may be too embarrassed to address their symptoms.
Prevention
Because scientific research is lacking, no specific information is available regarding prevention.
Resources
BOOKS
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th edition, text revised. Washington, DC: American Psychiatric Association,2000.
Keuthen, Nancy J., Dan J. Stein, and Gary A. Christenson. Help for Hair Pullers: Understanding and Coping with Trichotillomania. Oakland, CA: New Harbinger Publications, 2001.
Stein, Dan J., Gary A. Christenson, and Eric Hollander, eds. Trichotillomania. Washington, D.C.: American Psychiatric Press, Inc., 1999.
PERIODICALS
Diefenbach, Gretchen J., David Reitman, and Donald A. Williamson. "Trichotillomania: A Challenge to Research and Practice." Clinical Psychology Review 20, no. 3(2000): 289-309.
Elliot, Amy J. and R. Wayne Fuqua. "Trichotillomania: Conceptualization, Measurement, and Treatment." Behavior Therapy 31 (2000): 529-545.
ORGANIZATIONS
Trichotillomania Learning Center, Inc. 303 Potrero #51, Santa Cruz, CA 95060. (831) 457-1004. <http://www.trich.org> .
Sandra L. Friedrich, M.A.
My parents thought it would go away just like they thought my older sister's thumb sucking would. She sucked her thumb till she was in junior high and I never stopped twirling my hair. I go through periods of baldness on the left side of my head but I always make an effort to stop just before it looks really bad.
It's embarassing, makes me look like a ditz, but worst of all I have no idea when I am doing it half the time. Literally within seconds of being told to stop, I start up again. Fuck I just did it right now, the radio distracted me and I started up again. I can't even imagine how to stop this. I know I have a lot of anxiety but I am too afraid to go see someone and have them tell me it's no big deal, because then where will I be?
ANYWAYS, here's some advice that works. Whatever friends you are comfortable with, tell them about your habit and have them yell stop at you or hit you (not too hard) when you do it. I used to do this with my close high school friends :)
but yeah.. my main question is, Does the hair regrow pretty quickly, since i have a weird looking bald spot on the side of my head..
It started the summer of 3rd and 4th grade at my aunt's apartment in San Francisco. She appraised my math skills, became upset and stood over me with belts, closed and open fists while threatening me not to get the answers wrong.
When she would walk away I would sit at the table crying, and worrying about when my mother would come save me from this type of treatment because she didn't beat us, yell, and call us names like her three siblings did. While wondered about my mother I would rest my head upon my left hand and twirl my index finger and thumb through my small afro until I snagged a tangled knot and I would pull it out which eventually led me to discover the root that I played with first. That led to rubbing the hair and root on my mouth w to notice the change in texture between the hair and the attached root. Also, pulling the hair out was and still is almost always preceded with intense stress or a sore spot on my scalp... I remeber her once asking why there is so much hair on my book and table but not waiting for an answer.
Sometimes plucking the hair gives me a feeling of ecstacy, even now. I've gone years without an episode but lately, I have been shaving my entire head bald because I accidentally plucked multiple bald spots on the top and back of my head.
The embarrassment's there but I have to face the world anyway. I worry that people may fear I have a communicable disease. Medicated shampoos help with sore spots when stress is low so I dont pull for that reason.
I'm currently engaged in a 3 month negotiation with my employer for a wage increase and coincidentally I pulled out far too much hair from my scalp. When people stand behind me I think they are looking at my head in disgust, but I block it out eventually.
The pleasure and relief that comes from the pain of pulling my hair out is strange to me but it's just there. I try to stay busy and wash my hair often and that seems to help some. :)