Stroke

Definition
A stroke, also called a cerebral vascular accident (CVA), is the sudden death of cells in a specific area of the brain due to inadequate blood flow.
Description
A stroke occurs when blood flow is interrupted to a part of the brain, either when an artery bursts or becomes closed when a blood clot lodges in it. Blood circulation to the area of the brain served by that artery stops at the point of disturbance, and the brain tissue beyond that is damaged or dies. (Brain cells need blood to supply oxygen and nutrients and to remove waste products.) Depending on the region of the brain affected, a stroke can cause paralysis, loss of vision, speech impairment, memory loss and reasoning ability, coma, or death. The effects of a stroke are determined by how much damage occurs, and which portion of the brain is affected.
About a third of all strokes are preceded by transient ischemic attacks (TIAs), or mini-strokes, that temporarily interrupt blood flow to the brain. While TIAs cause similar symptoms (such as sudden vision loss or temporary weakness in a limb), they abate much more quickly than full-fledged strokes, usually within a few hours— sometimes as quickly as a few minutes.
Stroke is a medical emergency requiring immediate treatment. Prompt treatment improves the chances of survival and increases the degree of recovery that may be expected. A person who may have suffered a stroke should be seen in a hospital emergency room without delay. Treatment to break up a blood clot, the major cause of stroke, must begin within three hours of the stroke to be most effective. Improved medical treatment of all types of stroke has resulted in a dramatic decline in death rates in recent decades. In 1950 nine in ten stroke victims died, compared to slightly less than one in three today.
Causes and symptoms
Causes
There are four main types of stroke: cerebral thrombosis, cerebral embolism, subarachnoid hemorrhage, and intracerebral hemorrhage. Cerebral thrombosis and cerebral embolism, known as ischemic strokes, are caused by blood clots that block an artery supplying the brain, either in the brain itself or in the neck. They account for 70–80% of all strokes. Subarachnoid hemorrhage and intracerebral hemorrhage are hemorrhagic strokes that occur when a blood vessel bursts around or in the brain, either from trauma or excess internal pressure. Hypertension (high blood pressure) and atherosclerosis are usually contributing factors in these types of strokes.
CEREBRAL THROMBOSIS. Cerebral thrombosis, the most common type of stroke, occurs when a blood clot, or thrombus, forms within the brain itself, blocking blood flow through the affected vessel. This is usually due to atherosclerosis (hardening) of brain arteries, caused by a buildup of fatty deposits inside the blood vessels. Cerebral thrombosis occurs most often at night or early in the morning, and is often preceded by a TIA. Recognizing the occurrence of a TIA, and seeking immediate treatment, is an important step in stroke prevention.
CEREBRAL EMBOLISM. Cerebral embolism occurs when a blood clot from elsewhere in the circulatory system breaks free. If it becomes lodged in an artery supplying the brain, either in the brain or in the neck, it can cause a stroke. The most common cause of cerebral embolism is atrial fibrillation, which occurs when the upper chambers (atria) of the heart beat weakly and rapidly, instead of slowly and steadily. Blood within the atria does not empty completely, and may form clots that can then break off and enter the circulation. Atrial fibrillation is a factor in about 15% of all strokes, but this risk can be dramatically reduced with daily use of anticoagulant medication (such as Heparin or Coumadin).
SUBARACHNOID HEMORRHAGE. In this type of stroke, blood spills into the subarachnoid space between the brain and cranium. As fluid builds up, pressure on the brain increases, impairing its function. Hypertension is a frequent cause of these types of stroke, but vessels with preexisting defects, such as an aneurysm, are also at risk for rupture. Aneurysms are most likely to burst when blood pressure is highest, and controlling blood pressure is an important preventive strategy. Subarachnoid hemorrhages account for about 7% of all strokes.
INTRACEREBRAL HEMORRHAGE. Representing about 10% of all strokes, intracerebral hemorrhage affects vessels and tissue within the brain itself. As with subarachnoid hemorrhage, bleeding deprives affected tissues of blood supply, and the accumulation of fluid within the inflexible skull creates pressure on the brain that can quickly become fatal. Despite this, recovery may be more complete for a person who survives hemorrhage than for one who survives a clot, because the effects of blood deprivation are usually not as severe.
Risk factors
Risk factors for stroke involve:
- Age and sex— the risk of stroke increases with age, doubling for each decade after age 55. Men are more likely to have a stroke than women.
- Heredity— People with a family history of stroke have an increased risk of stroke themselves. In addition, African-Americans, Asians, and Hispanics all have higher rates of stroke than whites, related partly to higher blood pressure.
- Diseases— People with diabetes, heart disease (especially atrial fibrillation), high blood pressure, or prior stroke are at greater risk for stroke. Patients with one or more TIAs have ten times the risk.
- Other medical conditions— Stroke risk increases with obesity , high blood cholesterol, or high red blood cell count.
- Lifestyle choices— Stroke risk increases with cigarette smoking (especially if combined with the use of oral contraceptives), a sedentary lifestyle, alcohol consumption above two drinks per day, and/or the use of cocaine or intravenous drugs.
Symptoms
Knowing the symptoms of stroke is as important as knowing those of a heart attack. Patients with stroke symptoms should seek emergency treatment without delay, which may mean dialing 911 rather than their family physician. Specific symptoms of a stroke depend on the type, but all types share some characteristics in common.
An embolic stroke usually comes on quite suddenly and is intense right from the start, while symptoms of a thrombotic stroke come on more gradually. Symptoms for these ischemic strokes may include:
- blurring or decreased vision in one or both eyes
- severe headache, often described as "the worst headache of my life"
- weakness, numbness, or paralysis of the face, arm, or leg, usually confined to one side of the body
- dizziness, loss of balance or coordination, especially when combined with other symptoms
Hemorrhagic strokes are somewhat different. An intracranial hemorrhage exhibits any or all of the following symptoms:
- loss of consciousness
- altered mental state
- seizure
- vomiting or severe nausea
- extreme hypertension
- weakness, numbness, or paralysis, especially on one side of the body
- sudden, severe headache
Symptoms of a subarachnoid hemorrhage include:
- severe headache that begins suddenly
-
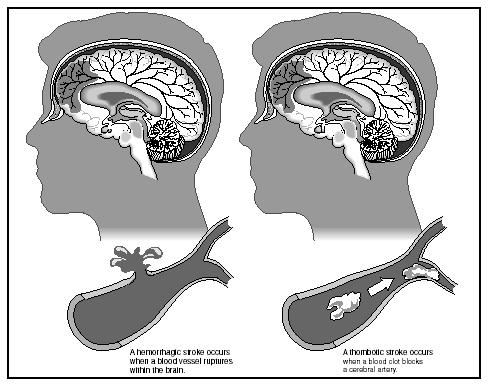 A hemorrhagic stroke (left) compared to a thrombotic stroke (right).(Illustration by Hans & Cassady, Inc.)
A hemorrhagic stroke (left) compared to a thrombotic stroke (right).(Illustration by Hans & Cassady, Inc.) - nausea or vomiting
- stiff neck
- light intolerance
- loss of consciousness
Demographics
Each year, more than half a million people in the United States have a stroke. It is the third leading cause of death, killing about a third of its victims—approximately 150,000 Americans each year. For those that survive, stroke is the leading cause of disability. Two-thirds of all strokes occur in people over age 65, with men more affected than women, although women are more likely to die from a stroke. African-Americans suffer strokes more often than whites, and are more likely to be die from them as well. This may be because African-Americans tend to suffer from hypertension more frequently than other groups.
Diagnosis
Diagnosing a stroke begins with a careful medical history, especially concerning the onset and distribution of symptoms, presence of risk factors; in this way other possible causes are excluded. A brief neurological exam is performed to identify the degree and location of any deficits, such as weakness, lack of coordination, or vision loss.
Once stroke is suspected, imaging technology is used to determine what type the patient has suffered—a critical distinction that guides therapy. A noncontrast computed tomography scan (CT scan) can reliably identify hemorrhagic strokes, caused by uncontrolled bleeding in the brain. Magnetic resonance imaging (MRI), on the other hand, particularly diffusion-weighted imaging, can detect ischemic strokes, caused by blood clots, earlier and more reliably than CT scanning.
Blood and urine tests are also run to look for possible abnormalities. Other investigations that may be performed to guide treatment include electrocardiogram, angiography, ultrasound, and electroencephalogram.
Treatment
When brain cells die during a stroke, they release toxic chemicals that can trigger a chain reaction that can injure or kill other nearby cells. Damage from stroke may be significantly reduced by emergency treatment, and is a significant factor in how fully a patient will recover.
Emergency treatment
Emergency treatment of an ischemic stroke attempts to dissolve the clot. This "thrombolytic therapy" is performed most often with tissue plasminogen activator (t-PA), which must be administered within three hours of the stroke event. (Patients who awaken with stroke symptoms are ineligible for this type of therapy, since the time of onset cannot be reliably determined.) t-PA therapy has been shown to improve recovery and decrease long-term disability in patients. It carries a 6.4% risk of inducing a cerebral hemorrhage, however, and is not appropriate for patients with bleeding disorders, very high blood pressure, known aneurysms, any evidence of intracranial hemorrhage, or incidence of stroke, head trauma, or intracranial surgery within the past three months. Patients with clot-related stroke who are ineligible for t-PA treatment may be treated with heparin or other blood thinners, or with aspirin or other anticlotting agents in some cases.
Emergency treatment of hemorrhagic stroke is aimed at controlling intracranial pressure that accompanies these types of strokes. New surgical techniques can effectively relieve the pressure, especially when begun soon after the stroke event occurs. Surgery for hemorrhage due to aneurysm may be performed if the aneurysm is close enough to the cranial surface to allow access. Ruptured vessels are closed off to prevent rebleeding. For aneurysms that are difficult to reach surgically, endovascular treatment, in which a catheter is guided from a larger artery up into the brain to reach the aneurysm, may be effective. Small coils of wire are discharged into the aneurysm, which plug it up and block off blood flow from the main artery.
Rehabilitation
Rehabilitation refers to a comprehensive program designed to regain as much function as possible and compensate for permanent losses. Approximately 10% of stroke survivors are without any significant disability and able to function independently. Another 10% are so severely affected that they must remain institutionalized for severe disability. The remaining 80% can return home with appropriate therapy, training, support, and care.
Rehabilitation is coordinated by a team of medical professionals and may include the services of a neurologist, a physician who specializes in rehabilitation medicine, a physical therapist, an occupational therapist, a speech-language pathologist, a nutritionist, a mental health professional, and a social worker. Rehabilitation services may be provided in an acute care hospital, rehabilitation hospital, long-term care facility, outpatient clinic, or at home.
The rehabilitation program is based on the patient's individual deficits and strengths. Strokes on the left side of the brain primarily affect the right half of the body, and vice versa. In addition, in left brain-dominant people, who constitute a significant majority of the population, left-brain strokes usually lead to speech and language deficits, while right-brain strokes may affect spatial perception. Patients with right-brain strokes may also deny their illness, neglect the affected side of their body, and behave impulsively.
Rehabilitation may be complicated by cognitive losses, including diminished ability to understand and follow directions. Poor results are more likely in patients whose strokes left them with significant or prolonged cognitive changes, sensory losses, language deficits, or incontinence.
PREVENTING COMPLICATIONS. Rehabilitation begins with prevention of medical complications, including stroke recurrence, using many of the same measures used to prevent stroke, such as smoking cessation and getting hypertension under control.
One of the most common medical complications following stroke is deep venous thrombosis, in which a clot forms within a limb immobilized by paralysis. Clots can also become lodged in an artery feeding the lungs, a condition called pulmonary embolism, that is a common cause of death in the weeks following a stroke. Resuming activity within a day or two after the stroke is an important preventive measure, along with use of elastic stockings on the lower limbs. Drugs that prevent clotting may also be given, including intravenous heparin and oral warfarin.
Weakness and loss of coordination of the swallowing muscles may impair swallowing (dysphagia), and allow food to enter the lower airway. This may lead to aspiration pneumonia, another common cause of death shortly after a stroke. Dysphagia may be treated with retraining exercises and temporary use of pureed foods.
Other medical complications include urinary tract infections, pressure ulcers, falls, and seizures . Not surprisingly, depression occurs in 30–60% of stroke patients; its severity is usually related to the level of permanent functional impairment It can be treated with anti-depressants and psychotherapy .
TYPES OF REHABILITATIVE THERAPY. Brain tissue that dies in a stroke cannot regenerate. In some cases, however, rehabilitation training can help other brain regions perform the same functions of that tissue. In other cases, compensatory actions may be developed to replace lost abilities.
Physical therapy is used to maintain and restore range of motion and strength in affected limbs, and to maximize mobility in walking, wheelchair use, and transferring (from wheelchair to toilet or from standing to sitting, for instance). The physical therapist advises patients on mobility aids such as wheelchairs, braces, and canes. In the recovery period, a stroke patient may develop muscle spasticity and contractures (abnormal muscle contractions) that can be treated with a combination of stretching and splinting.
Occupational therapy improves self-care skills such as feeding, bathing, and dressing, and helps develop effective compensatory strategies and devices for activities of daily living. A speech-language pathologist focuses on communication and swallowing skills. When dysphagia is a problem, a nutritionist can advise alternative meals that provide adequate nutrition.
Psychological therapy can help treat depression or loss of thinking (cognitive) skills. A social worker may help coordinate services and ease the transition out of the hospital back into the home. Both social workers and mental health professionals help counsel the patient and family during the difficult rehabilitation period. Caring for a person affected with stroke requires a new set of skills and adaptation to new demands and limitations. Home caregivers may develop stress , anxiety, and depression—caring for the caregiver is an important part of the overall stroke treatment program. Support groups can provide an important source of information, advice, and comfort for stroke patients and caregivers; joining one can be an important step in the rehabilitation process.
Prognosis
Stroke is fatal for about 27% of white males, 52% of African-American males, 23% of white females, and 40% of African-American females. Stroke survivors may be left with significant deficits. Emergency treatment and comprehensive rehabilitation can significantly improve both survival and recovery.
Prevention
The risk of stroke can be reduced through lifestyle changes:
- stop smoking
- control blood pressure
- get regular exercise
- maintain a healthy weight
- avoid excessive alcohol consumption
- get regular checkups and follow the doctor's advice regarding diet and medicines
Use of high-estrogen dose oral contraceptives increase the chances for developing stroke, particularly in women who smoke and/or who are over 35. Currently, there are low-estrogen dose oral contraceptives, for which a clear relationship with stroke development is unclear.
Treatment of atrial fibrillation may also significantly reduce the risk of stroke. Preventive anticoagulant therapy may benefit those with untreated atrial fibrillation. Warfarin (Coumadin) has proven to be more effective than aspirin for those with higher risk.
Screening for aneurysms may be an effective preventive measure in those with a family history of aneurysms or autosomal polycystic kidney disease, which tends to be associated with aneurysms.
Resources
BOOKS
Caplan, L. R., M. L. Dyken, and J. D. Easton. American Heart Association Family Guide to Stroke Treatment, Recovery, and Prevention. New York: Times Books, 1996.
Duthie, Edmund H., Jr. Practice of Geriatrics. 3rd Edition. Philadelphia: W. B. Saunders, 1998: 328-335.
Goetz, Christopher G., and others. Textbook of Clinical Neurology. 1st edition. Philadelphia: W. B. Saunders, 1999: 909-911.
Warlow, C. P., and others. Stroke: A Practical Guide to Management. Boston: Blackwell Science, 1996.
PERIODICALS
Krishnan, K. Ranga Rama. "Depression as a contributing factor in cerebrovascular disease." American Heart Journal 140 (October 2000): 563.
ORGANIZATIONS
American Heart Association and American Stroke Association. 7272 Greenville Ave. Dallas, TX 75231.(214) 373-6300. <http://www.americanheart.org> .
National Stroke Association. 9707 E. Easter Lane, Englewood, Co. 80112. (800) 787-6537. <http://www.stroke.org> .
Laith Farid Gulli, M.D. Bilal Nasser, M.D.
Comment about this article, ask questions, or add new information about this topic: