Obesity
Definition
Obesity is the condition of having an excessive accumulation of fat in the body, resulting in a body weight more than 20% above the average for height, age, sex, and body type, and in elevated risk of disability, illness, and death.
Description
The human body is composed of bone, muscle, specialized organ tissues, and fat. Together, all of these tissues comprise the total body mass, which is measured in pounds. Fat, or adipose tissue, is a combination of essential fat (an energy source for the normal physiologic function of cells and organs) and storage fat (a reserve supply of energy for future needs). When the amount of energy consumed as food exceeds the amount of energy expended in the normal maintenance of life processes and in physical activity, storage fat accumulates in excessive amounts. Essential fat is tucked in and around internal organs, and is an important building block of all cells in the body. Storage fat accumulates in the chest and abdomen, and, in much greater volume, under the skin.
Causes and symptoms
The human body was designed for life forty thousand years ago, when the ability to store energy in times of plenty meant the difference between life and death during famine. This protective mechanism is a source of trouble when food, in unlimited quantities, is readily available,. This is evident in the increasing prevalence of obesity in modern times, particularly in Western cultures. While obesity is just an exaggeration of a normal body, the storage of energy for future is properly classified as a health problem. This is because excessive amounts of storage fat may interfere with the normal physiology of the body. Obesity is directly related to the increasing prevalence of Type II diabetes in American society and for the appearance of Type II diabetes in children, previously a rarity. Because obesity promotes degenerative disease of joints and heart and blood vessels, it increases the need for some surgical procedures. At the same time, surgical complication rates are higher in obese patients. Obesity contributes to fatigue , high blood pressure, menstrual disorders, infertility, digestive complaints, low levels of physical fitness, and to the development of some cancers. The social costs of obesity that include decreased productivity, discrimination, depression, and low self-esteem, are less easily described and measured. Worldwide, obesity has reached epidemic proportions in the last thirty years, affecting both sexes and all ethnic, age, and socioeconomic groups. More than 50% of adults in the United States currently fall into overweight or obese classifications, and 22% of preschool children are classified as overweight. The increasing prevalence of obesity and diabetes in children and young adults heralds spiraling health care costs in the near future.
Because obesity reflects an imbalance between the amount of energy taken into the body in the form of food and the amount of energy expended in metabolism and physical activity, and because eating is an activity that involves choice and volition, obesity is classified by the Health Care Financing Administration (HCFA) as a "behavior" rather than as a disease. In recent years, following a pattern established in other behavioral problems such as alcoholism, researchers have attempted to establish a biologic basis for the development of obesity. They have succeeded in identifying many markers of the biochemical mechanisms that appear to be involved in feedback loops that control energy balance. However, much of the information is extrapolated from experimental work in rodents. Leptin, a hormone produced in fat cells is an example of such a marker. Leptin excited a great deal of hope as a potential treatment of obesity, but, as with many other laboratory discoveries, the hormone has proved far more complex and less easily understood in humans. Research to date indicates that obesity is the end product of numerous contributing factors, including genetics, hormonal influences, behavioral tendencies, medication effects, and the surrounding society. But the rapid and widespread increase in obesity in the last thirty years reflects changes in activity patterns and in eating habits, not a change in the human genetic pool or in physiology.
Diagnosis
There are two methods of diagnosing obesity. The first method is inspection—whereby an excessive amount of storage fat is usually noticeable upon visual inspection. The second method is inference of body fat content, obtained from body measurements such as weight or skinfold thickness, and comparison with charts of similar measurements in broad populations. The determination of obesity is based on the amount of variance from "normal," a value that comes from statistics on death rates in people with similar measurements. Calculations such as the body mass index (BMI) use a height-weight relationship to calculate an individual's ideal weight and personal risk of developing obesityrelated health problems. An individual with a BMI of25.9–29, for example, is considered overweight; a person with a BMI over 30 is classified as obese.
The problem with using weight as a measure of obesity is the fact that weight does not accurately represent body composition. A heavily-muscled football player may weigh far more than a sedentary man of similar height, but have significantly less body fat. Chronic dieters, who have lost significant muscle mass during periods of caloric deprivation, may look slim and weigh little, but have elevated body fat percentages. The most accurate means of estimating body fat content involves weighing a person two ways: First, the person is weighed under water. The difference between dry and underwater weight is calculated to obtain the volume of water displaced by the mass of the body. While this method is impractical, it has the advantage of determining body composition most accurately, and is the truest reflection of the actual percentage of body mass that is fat. Women whose body fat exceeds 30% of total body mass and men whose body fat exceeds 25% are generally considered obese.
The pattern of fat distribution on the body may indicate whether an individual has a predisposition to develop certain diseases or conditions that may accompany obesity. "Apple-shaped" individuals who store most of their weight around the waist and abdomen are at greater risk for cancer, heart disease, stroke , and diabetes than "pear-shaped" people, whose extra pounds settle primarily on their hips and thighs.
Treatment
Since obesity develops when intake of the food required to produce energy exceeds the amount of energy used in metabolism and in physical activity, the treatment of obesity must alter one or both aspects of the energy stream. The options are to decrease energy intake or to increase energy output, or both. However, the problem does not yield rapidly to either method. Storage fat is meant to protect its bearer from starvation when food is unavailable, and before fat is tapped for energy. In the face of decreased intake of food, the body breaks down muscle to construct the sugar it needs to feed the brain . Much of the early weight loss on a very low calorie diet represents loss of muscle tissue rather than loss of fat. Similarly, fat
When obesity develops in childhood, the total number of fat cells increases (hyperplastic obesity), whereas in adulthood, it is the total amount of fat in each cell that increases (hypertrophic obesity). Decreasing the amount of energy (food) consumed or increasing the amount of energy expended cannot change the number of fat cells already present. These actions can only reduce the amount of fat in each cell, and only if the process is slow and steady—as it was in reverse, when the excess fat accumulated. Prevention, as in so many problems, is far superior to any available treatment of obesity.
The strategy for weight loss in obese patients is first to change behavior; then, it is to decrease the expectation of rapid change. Behavioral treatment is goal-directed, process-oriented, and relies heavily on self-monitoring. Emphasis is on:
- Food intake: The potential energy provided by food is measured in calories, and the capacity of a certain type and amount of food to provide energy is called its caloric content. Keeping a food diary and developing a better understanding of the nutritional value and fat content of foods, changing grocery-shopping habits, paying attention to timing and appearance of meals, and slowing the speed of eating all help to modify food intake.
- Response to food: The body is capable of matching energy intake and output perfectly, but, in obese individuals, food intake is often unrelated from physiologic cues. Eating occurs for many reasons other than hunger. What psychological issues underlie the eating habits? Does stress cause binge eating ? Is food seen as a reward? Recognition of psychological triggers is necessary for the development of alternate coping mechanisms that do not focus on food.
- Time usage: The body is suited for an ancient world in which physical activity was a necessity. In the modern world, physical activity must be a conscious choice. Making activity and exercise an integrated part of everyday life is a key to achieving and maintaining weight loss. Sedentary and overweight individuals have to reclaim slowly the endurance that is natural by managing their time to allow for gradual increases in both programmed and conscious lifestyle activity.
Behavior modification
For most individuals who are mildly obese, behavior modifications entail life-style changes they can make independently if they have access to accurate information and have reached the point of readiness to make a serious commitment to losing weight. A family physician's evaluation is helpful, particularly in regard to exercise capacity and nutritional requirements. Commercial weight-loss programs may be helpful for some mildly obese individuals, but they are of varying quality. A good program emphasizes realistic goals, gradual progress, sensible and balanced eating, and increased physical activity; it is often recommended by physicians. Programs that promise instant weight loss or feature severe restrictions in types and amounts of food are not effective, and, in some cases, can be dangerous.
For individuals who are moderately obese, medically supervised behavior modification and weight loss are more likely to be effective than an independent program. A realistic goal is loss of 10% of current weight over a six-month period. While doctors put most moderately obese patients on balanced, low-calorie diets (1,200–1,500 calories a day), occasionally they recommend a very low calorie liquid protein diet (400–700 calories), with supplementation of vitamins and minerals, for as long as three months. Professional help with behavior modification is of paramount importance in such cases; without changing eating habits and exercise patterns, weight lost will be regained quickly.
Surgery
For individuals who are morbidly obese, surgery to bypass portions of the stomach and small intestine may at times be the only effective means of producing sustained and significant weight loss. Such obesity surgery, however, can be risky, and it is performed only on patients for whom other strategies have failed and whose obesity seriously threatens health. Liposuction is a purely cosmetic procedure in which a suction device is used to remove fat from beneath the skin, and has no place in the treatment of obesity.
Medications
Most of the current research on obesity is aimed at identifying biochemical pathways that will be amenable to intervention with drug treatments. These medications would be specifically tailored to interfere with the energy cycles to facilitate weight loss. As of 2002, there are two major classes of drugs that are approved for the treatment of obesity by the U.S. Food and Drug Administration (FDA). History of the field is littered with drugs that have failed or that have caused serious side effects. Appetite suppressant drugs such as Dexatrim and Meridia (sibutramine) change the amounts of some neurotransmitters in the brain. These chemical changes result in decreased appetite, but only in the presence of the drug. Digestive inhibitors such as Orlistat (Xenical) are drugs that interfere with the breakdown and absorption of dietary fat in the intestines; they are, however, poorly tolerated by the person who is obese because the effects of fat malabsorption are unpleasant.
These drugs also interfere with the absorption of some necessary vitamins. Fat substitutes such as Olestra, while technically not drugs, attempt to recreate the pleasant taste that fat adds to food, but create the same negative side effects as digestive inhibitors. Unless an obese individual has also made necessary behavioral changes, excess weight returns quickly when appetite suppressants or malabsorptive agents are stopped.
The use of any drug is associated with unwanted side effects, so that the decision to take a drug must come after the potential side effects are weighed against the potential benefits. No drug, current or past, has had such dramatic effects on obesity that it warrants its casual use. While most of the immediate side effects that may occur are reversible, the long-term effects, in many cases, are unknown. Even after a new drug successfully negotiates the stringent FDA approval process, its widespread use over a longer time frame may lead to the side effects that were not initially observable in the test population. Two popular obesity drugs of the early 1990s have already been withdrawn from the market because of unanticipated and severe cardiac problems. Meridia, just released in 1997, is already under scrutiny by a consumer group for its relationship to several deaths. Nevertheless, studies show that when obesity drugs are combined with behavioral changes—and especially with a portion controlled diet—weight loss is significantly greater than in a control group treated with behavior modification alone, at least after six months. It remains to be proved whether drug-assisted weight loss is long lasting.
Alternative treatment
The Chinese herb, ephedra ( Ephedra sinica ), combined with caffeine, exercise, and a low-fat diet, can cause a temporary increase in weight loss, at best. However, ephedra and caffeine are both central nervous system (CNS) stimulants, and the large doses of ephedra required to achieve the weight loss can also cause anxiety, irritability, and insomnia . Further, ephedra has been implicated in more serious conditions, such as seizure and stroke. Ephedra should not be used by anyone with a history of diabetes, heart disease, or thyroid problems.
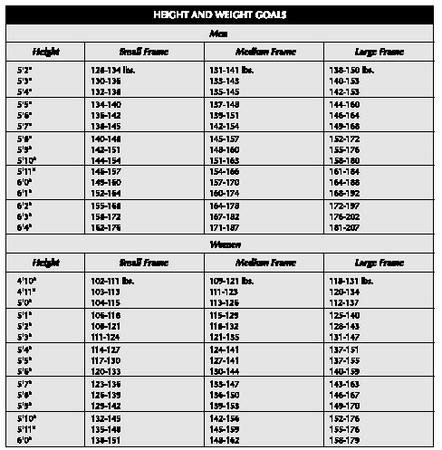
| HEIGHT AND WEIGHT GOALS | |||
| Men | |||
| Height | Small Frame | Medium Frame | Large Frame |
| 5′2″ | 128-134 lbs. | 131-141 lbs. | 138-150 lbs. |
| 5′3″ | 130-136 | 133-143 | 140-153 |
| 5′4″ | 132-138 | 135-145 | 142-153 |
| 5′5″ | 134-140 | 137-148 | 144-160 |
| 5′6″ | 136-142 | 139-151 | 146-164 |
| 5′7″ | 138-145 | 142-154 | 149-168 |
| 5′8″ | 140-148 | 145-157 | 152-172 |
| 5′9″ | 142-151 | 148-160 | 155-176 |
| 5′10″ | 144-154 | 151-163 | 158-180 |
| 5′11″ | 146-157 | 154-166 | 161-184 |
| 6′0″ | 149-160 | 157-170 | 164-188 |
| 6′1″ | 152-164 | 160-174 | 168-192 |
| 6′2″ | 155-168 | 164-178 | 172-197 |
| 6′3″ | 158-172 | 167-182 | 176-202 |
| 6′4″ | 162-176 | 171-187 | 181-207 |
| Women | |||
| Height | Small Frame | Medium Frame | Large Frame |
| 4′10″ | 102-111 lbs. | 109-121 lbs. | 118-131 lbs. |
| 4′11″ | 103-113 | 111-123 | 120-134 |
| 5′0″ | 104-115 | 113-126 | 112-137 |
| 5′1″ | 106-118 | 115-129 | 125-140 |
| 5′2″ | 108-121 | 118-132 | 128-143 |
| 5′3″ | 111-124 | 121-135 | 131-147 |
| 5′4″ | 114-127 | 124-141 | 137-151 |
| 5′5″ | 117-130 | 127-141 | 137-155 |
| 5′6″ | 120-133 | 130-144 | 140-159 |
| 5′7″ | 123-136 | 133-147 | 143-163 |
| 5′8″ | 126-139 | 136-150 | 146-167 |
| 5′9″ | 129-142 | 139-153 | 149-170 |
| 5′10″ | 132-145 | 142-156 | 152-176 |
| 5′11″ | 135-148 | 145-159 | 155-176 |
| 6′0″ | 138-151 | 148-162 | 158-179 |
Diuretic herbs, which increase urine production, can cause short-term weight loss, but cannot help patients achieve lasting weight control. The body responds to heightened urine output by increasing thirst to replace lost fluids, and patients who use diuretics for an extended period of time retain water even in the presence of the diuretic. In moderate doses, psyllium, a mucilaginous herb available in bulk-forming laxatives like Metamucil, absorbs fluid and makes patients feel as if they have eaten enough. Red peppers, mustard, and dandelion are said to generate weight loss by accelerating the metabolic rate. Dandelion also counteracts the desire for sweet foods. Walnuts contain serotonin, the brain chemical that signals satiety.
Acupressure and acupuncture can also suppress food cravings. Visualization and meditation can create and reinforce a positive self-image that enhances determination to lose weight. By improving physical strength, mental concentration and emotional serenity, yoga can provide the same benefits.
The correct balance of the basic food groups is also important, and believed by some experts to enhance the metabolic rate.
Prognosis
As many as 85% of dieters who do not exercise on a regular basis regain their lost weight within two years. In five years, the figure rises to 90%. Repeatedly losing and regaining weight (yo-yo dieting) encourages the body to store fat and may increase a patient's risk of developing heart disease. The primary factor in achieving and maintaining weight loss is a lifelong commitment to regular exercise and sensible eating habits.
Prevention
Obesity experts suggest that a key to preventing excess weight gain is monitoring fat consumption rather than counting calories; in fact, the National Cholesterol Education Program maintains that only 30% of calories should be derived from fat. Only one-third of those calories should come from saturated fats (the kind of fat found in high concentrations in meat, poultry, and dairy products). However, total caloric intake cannot be ignored, since it usually the slow accumulation of excess caloric intake, regardless of its source, that results in obesity. Erring on the side of 25 excess calories a day, a single cookie will result in a five-pound weight gain by the end of a year. Without recognition of the problem, weight balloons up another 45 pounds by the end of 10 years, and the return to normal weight is an arduous process. Because most people eat more than they think they do, keeping a detailed and honest food diary is a useful way to recognize eating habits. Eating three balanced, moderate-portion meals a day—with the main meal at mid-day—is a more effective way to prevent obesity than fasting or crash diets, which convince the body that there is an ongoing famine. After 12 hours without food, the body has depleted its stores of readily available energy, and hunkers down to begin protecting itself for the long term. Metabolic rate starts to slow, and breakdown of muscle tissue for the raw materials needed for energy maintenance begins. Until more food appears, famine mode persists and deepens; when the fast is lifted, the body is in a state of slowed metabolism, has a bit less muscle, and requires less food than before the fast. Exercise increases the metabolic rate by creating muscle, which burns more calories than fat. When regular exercise is combined with consistent, healthful meals, calories continue to burn at an accelerated rate for several hours.
Finally, encouraging healthful habits in children is a key to preventing childhood obesity and the health problems that follow in adulthood.
Resources
BOOKS
Aronne, Louis J. "Obesity and Weight Management." In Textbook of Primary Care Medicine. 3rd ed. Edited by John Noble, M.D. St. Louis, MO: Mosby, 2001.
The Editors of Time-Life Books. The Medical Advisor: The Complete Guide to Alternative & Conventional Treatments. Alexandria, VA: Time Life, Inc. 1996.
Harris, Dan R., ed. Diet and Nutrition Sourcebook. Detroit, MI: Omnigraphics, 1996.
Wilmore, Jack H. and David L. Costill. "Obesity, Diabetes, and Physical Activity." In Physiology of Sport and Health. 2nd ed. Champaign, IL: Human Kinetics, 1999.
PERIODICALS
Jensen, Michael D., ed. "Obesity." Medical Clinics of North America 84, no.2 (March 2000): 305–518.
Lustig, Robert H. "The Neuroendocrinology of Obesity." Endocrinology and Metabolism Clinics 30, no. 3 (September 2001): 765–785.
Patel, Manesh R. and Darren K. McGuire. "Pounds of Prevention." American Heart Journal 142, no.3 (September 2001): 388–90.
Rocchini, Albert P. "Childhood Obesity and A Diabetes Epidemic." New England Journal of Medicine 346, no. 11 (March 14, 2002): 854–855.
ORGANIZATIONS
American Dietetic Association. 216 West Jackson Blvd., Chicago, IL 60606-6995. <http://www.eatright.org> .
American Obesity Association. 1250 24th St. NW, Washington D.C. 20037. <http://www.obesity.org> .
Shape Up America. 6707 Democracy Blvd., Suite 306, Bethesda, MD 20817. <http://www.shapeup.org/general/index.html> .
Weight-Control Information Network. 1 Win Way, Bethesda, MD 20892-3665. <http://www.niddk.nih.gov/health/nutrit/win.html> .
Elizabeth Reid, M.D.
Comment about this article, ask questions, or add new information about this topic: